

Timing of therapy
Current Australian Guidelines advise treating all people with HIV infection as soon as possible regardless of CD4 count 40 Selecting a cART regimen may also be influenced by the particular treatment regimen being considered for HCV (see below).
The decisions regarding the timing of HCV therapy were previously quite complex due to the toxicity of interferon / ribavirin treatment. However, with the arrival of well-tolerated, highly effective treatment it is now recommended to treat all patients with HIV- HCV coinfection. In general HIV should be fully suppressed prior to HCV treatment.
Initial investigations
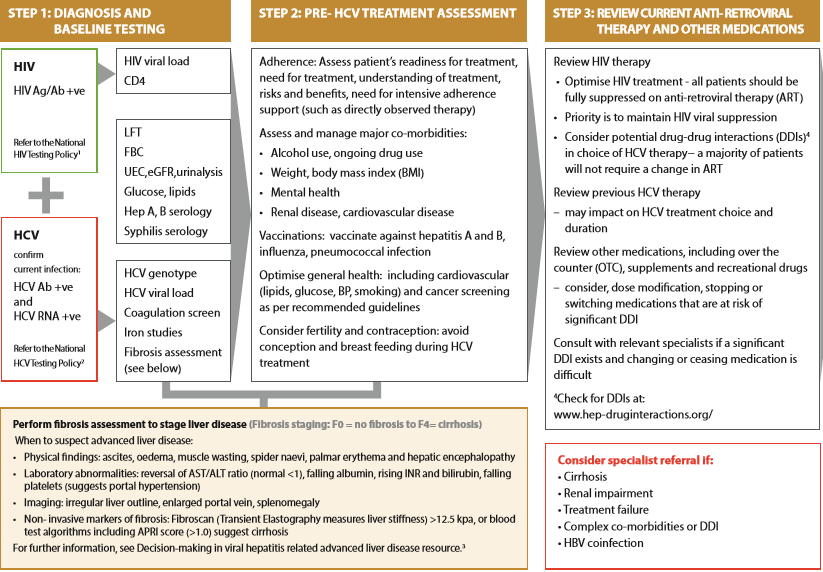
Table X shows a pathway for the initial assessment of HIV-HCV coinfected patients.
Aim of HCV treatment
The aim of HCV therapy is the eradication of HCV RNA from serum. This is referred to as a sustained virological response (SVR12), or cure, and is defined as undetectable serum HCV RNA 12 weeks after completion of therapy.
Treatment selection
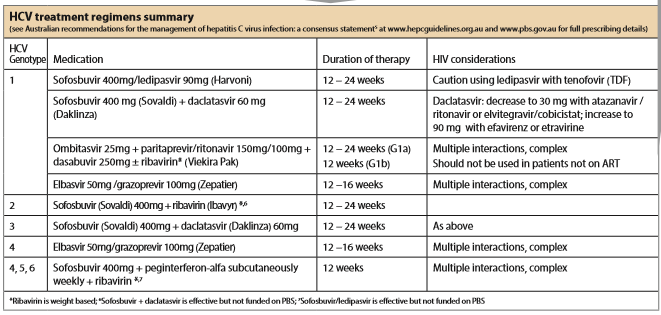
Australian recommendations for the management of hepatitis C virus infection: a consensus statement (January 2017) provides recommended treatment regimens for HCV-HIV co-infection.41 In general these are the same as for HCV mono-infection with comparable outcomes. (see table X).
The possibility of drug-drug interactions should be assessed prior to treatment using the University of Liverpool’s Hepatitis Drug Interactions website (www.hep-druginteractions.org). Many ARVs have significant interactions. This may result in the selection of alternative DAA regimens or in dose modification of DAA therapy.
DAA therapy is constantly evolving. ‘Pangenotypic’ therapy with several new agents is likely to be available in Australia in the near future.
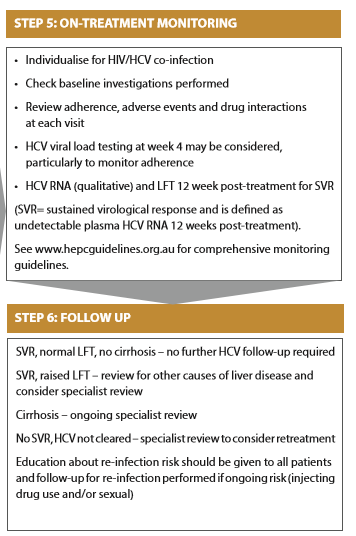
Monitoring during and after DAA treatment
Patients require limited monitoring during treatment due to the low toxicity of DAA therapy. (see table X). Similarly monitoring post treatment is straightforward. The small number of patients who fail to clear HCV need specialist review regarding retreatment with newer DAA therapy. Patients with ongoing abnormal liver function also need specialist evaluation regarding other causes of liver disease.
Summary:
HCV-HIV coinfection is common and has historically contributed to the heavy burden of comorbidity and premature mortality for this population. The recent arrival of effective HCV treatment now offers a cure for the vast majority of those living with HCV infection.